When Your Child Has Vesicoureteral Reflux
Your child has been diagnosed with vesicoureteral reflux (VUR). This condition affects the urinary tract. VUR often does not cause pain and it can be treated or managed. In some cases, children even outgrow the condition. Your child’s healthcare provider will tell you more about choices for your child.
What is VUR?
A tube called the ureter carries urine from each kidney to the bladder. Normally, the connection valve where the ureter and bladder meet helps move urine out of the body. With VUR, the connection valve doesn’t close correctly so it allows urine to flow backward (reflux). Bacteria from the bladder can enter the kidneys and cause infection or damage.
What causes VUR?
The connection where the ureter and bladder meet didn’t form normally while your child was growing in the womb. It's not known why this happened. What is known is that you did nothing to cause VUR in your child. Certain factors may make VUR more likely to happen in some children. One of these is family history. If you or someone in your family had VUR, your children may be more likely to have it. Your child’s healthcare provider may suggest that your other children be screened for reflux.
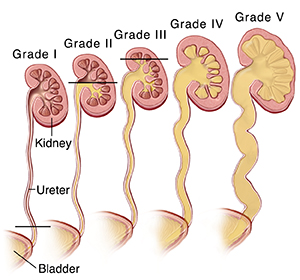 |
| With VUR, urine flows backward from the bladder into the ureter (refluxes) and can cause the ureter and kidney to swell. Grades I-V are given depending on the severity of the reflux. |
Grading of reflux
The reflux grading system is used to determine how severe the reflux is. The higher the grade, the more severe the reflux. In severe cases, reflux is less likely to go away on its own.
-
Grade I: Urine refluxes into the ureter only.
-
Grade II: Urine refluxes into the ureter and enters the renal (kidney) pelvis.
-
Grade III: Reflux starts to cause the ureter and calyces (parts of the kidney that collect the urine and drain into the bladder) to swell (dilate).
-
Grade IV: The ureter and calyces appear more dilated than with Grade III. This causes moderate swelling.
-
Grade V: The ureter and renal pelvis are severely dilated. The severe reflux also causes the shape of the calyces to change. The entire kidney becomes enlarged.
What are the signs of VUR?
VUR may cause no symptoms, or may have signs including:
-
History of kidney infections
-
Fever of 100.4°F (38°C) or higher, or as directed by your child's healthcare provider, because of a urinary tract infection (UTI)
-
Swelling of one or both ureters and kidneys
How is VUR diagnosed?
VUR may have been seen in your unborn child during a routine ultrasound. The baby’s kidneys or ureters looked abnormal. Or, VUR may have been suspected if your newborn or child had a UTI. To gather more information about your child’s health, the healthcare provider will ask you questions. A physical exam will also be done to look for problems. To help get more information, the following tests may be done:
-
Urine tests to check for a UTI or protein in the urine. Protein in the urine can be a sign of kidney disease.
-
A kidney ultrasound to look for kidney swelling.
-
A voiding cystourethrogram (VCUG) to determine if reflux is happening and rule out functional disorders. The test allows the healthcare provider to grade how severe the reflux is.
-
Radionuclide cystography to help detect reflux.
-
A radionuclide renal scan to determine if scarring of kidneys has occurred. The test also allows the healthcare provider to see how well each kidney works.
How is VUR treated?
Treatment depends on the child’s age, grade of reflux, frequency of infections, and whether the kidneys have scarring. Often, the goal of treatment is to prevent kidney infections while waiting for the child to outgrow the condition. In some cases, surgery may be needed to fix reflux. While waiting for your child to outgrow VUR or have surgery for it, they may need to:
-
Take a daily low-dose antibiotic (medicine to prevent infection)
-
Have follow-up tests as often as instructed
-
Be treated for constipation
-
Practice timed voiding if the child is potty trained (see below)
Timed voiding
Timed voiding means urinating at scheduled times. It allows potty-trained kids to empty their bladders on a regular basis. This helps prevent infections and avoid wetting accidents. To practice timed voiding, your child will need to visit the bathroom at set times throughout the day. Their healthcare provider can suggest how often your child should urinate. Your child should NOT wait until the urge to urinate arises if they have a voiding dysfunction.
What are the long-term concerns?
In many cases, VUR goes away by itself. This is because the connection between the ureter and the bladder develops more and works better as the child grows. Bladder control also improves as your child gets older. If VUR isn’t treated, the risk of kidney infection and damage is increased. Your child’s healthcare provider can tell you more about concerns for your child.